


Heart and circulatory system
Normal structure and function

This post is part of a series on the normal functioning of the human body. Here we think about the structure and function of the heart and circulatory system. An understanding of the basic anatomy and physiology of the body is essential in order to develop an understanding of how the body goes wrong in disease processes.
Basic structure of the heart
The heart is a hollow organ located in the centre, and extending to the left of, the thoracic cavity. With the sternum and ribs to the front and the thoracic spinal column behind, the heart is well protected from physical trauma. Within the heart there are four chambers. The two upper chambers are termed atria and the lower chambers ventricles. These chambers are simply named according to the side of the heart they are on, so they are the right and left atria, and the right and left ventricles. Valves separate the atria from the ventricles and the ventricles from the aorta and pulmonary artery. The left and right sides of the heart are separated by the cardiac septum. This means that blood from the right side cannot mix with blood from the left side and vice versa.

Diagram 2.1 The basic structures of the heart. The muscular wall of the left ventricle is thicker than that of the right ventricle. The walls of the atria are relatively thin.
The wall of the heart is in three layers
The inner layer of the heart is called the endocardium and is composed of smooth squamous epithelium. When an epithelium is lining internal structures, it is referred to as an endothelium. This endothelium allows the smooth uninterrupted flow of blood through the heart. Endocardium also covers the heart valves. The importance of the smooth lining provided by the endocardial endothelium is highlighted if it becomes infected, a condition termed endocarditis. Usually caused by a Streptococcus, this condition causes inflammation of the endothelium followed by deposits of the blood clotting protein fibrin, causing the build up of ‘vegetation’. If this material is dislodged it will enter the circulatory system as emboli which can lodge in the small arterial supply of any part of the body.
The myocardium is the middle layer of the heart wall and is composed of specialised cardiac heart muscle. All of the energy for the pumping action of the heart is generated by the contraction of the myocardium. This cardiac form of muscle is only found in the heart and is composed of specialised cells called cardiomyocytes. Myocardial muscle is striped or striated in nature but, unlike skeletal muscle, is involuntary. As the myocardium must contract approximately 72 times per minute it uses a lot of nutrients and oxygen.
The outer layer of the heart is termed the pericardium and is composed of two layers. An inner layer is composed of serous membrane which is adherent to the outside of the myocardium. This is referred to as the visceral pericardium or epicardium. The outer pericardial layer is composed of tough fibrous tissue, which is itself lined internally with another layer of serous membrane. A serous membrane is a membrane which secretes serous lubrication fluid, in this case to allow the heart to move within the fibrous pericardial sac with minimal friction between layers. This allows the heart to expand and contract smoothly during a normal cardiac cycle. The fibrous layer is protective and prevents the heart over expanding. If fluid or blood collects under the fibrous pericardium the pressure can squash the heart and may cause death. This condition is termed cardiac tamponade.

Diagram 2.2 The three layers which compose the wall of the heart, endocardium, myocardium and pericardium.
Heart valves ensure one way flow of blood
Valves are essential to control the direction of blood flow through the heart, opening and closing as a result of pressure changes in the blood. A valve will only allow the blood to flow in one direction.
The atria and ventricles are separated by valves collectively referred to as atrioventricular valves. On the right side, the atrioventricular valve is called the tricuspid valve. This is because it is made up of three separate cusps. The bicuspid valve is between the left atrium and ventricle and is composed of two cusps. Often the bicuspid valve is referred to as the mitral valve as an alternative name. These valves allow the free flow of blood from the atria into the ventricles but close during ventricular contraction to prevent blood passing from the ventricles back into the atria.
Atrioventricular valves are attached to the ventricular wall by strong tendons called chordae tendineae or tendonous cords. These prevent the valves opening upwards, i.e. the wrong way. The tendonous cords are themselves connected to the wall of the heart via specialised muscle bundles called papillary muscles. Papillary muscles contract at the same time as the ventricular wall. As they contract, they pull on the tendonous cords which tightly close the valves, preventing any possible regurgitation of blood from the ventricles back into the atria.

Diagram 2.3 (i) View of the closed tricuspid valve from above. (ii) View of the closed bicuspid (mitral) valve from above.
Between the left ventricle and the aorta is the aortic valve (in some texts you may see this referred to as the aortic semilunar valve). Between the right ventricle and the pulmonary artery is the pulmonary valve (also sometimes referred to as the pulmonary semilunar valve). When the ventricles are contracting the aortic and pulmonary valves open to allow the free flow of blood into the aorta and pulmonary artery. At the end of ventricular contraction these valves close to prevent blood flowing from the aorta and pulmonary artery back into the ventricles.
Cardiac massage is a technique that can be used when the heart is not able to contract independently. This takes advantage of the valves within the heart only allowing blood to flow in the correct physiological direction through the heart. In cardiac massage the heart is compressed between the thoracic vertebral column and the sternum. As the pressure in the heart increases, blood will open the valves and be forced through the heart and out into the aorta and pulmonary artery. Good cardiac massage will therefore generate a cardiac output which may be detected as a central pulse. This cardiac output will perfuse the vital organs of the body such as the lungs, brain, kidneys and the heart itself. This can be maintained until additional treatments restore a normal cardiac rhythm.
Blood flow through the heart
The heart is the pump which generates the flow of blood through the arterial and capillary systems of the body.
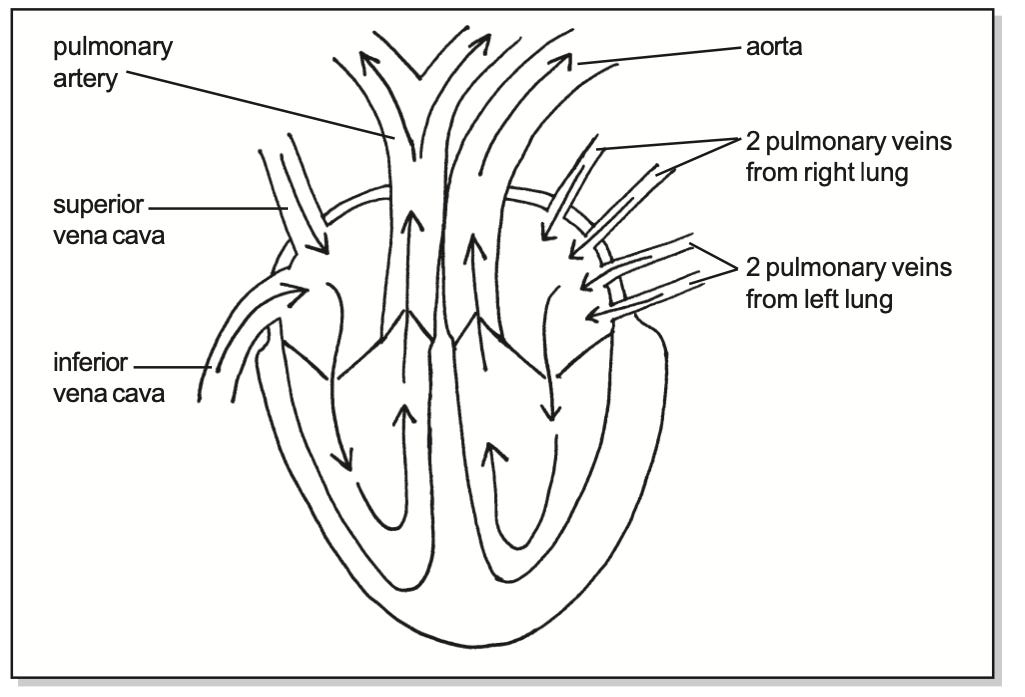
Diagram 2.4 The major blood vessels associated with the heart. Arrows indicate direction of blood flow.
Atrial function
Atria act as receiving chambers for the venous blood which is returning to the heart via the large veins. When the ventricles are not contracting blood returning to the heart, via the large veins, will pass directly through the atria, through the atrioventricular valves and will start filling up the ventricles.
However, when the ventricles are contracting blood returning to the atria will not be able to pass directly into the ventricles. Therefore, during ventricular contraction returning blood is stored in the atria. Once the ventricles have completed a contraction, the atrioventricular valves will open and the blood stored in the atria will rapidly pass into the ventricles. One tenth of a second before the onset of the next ventricular contraction, when the ventricles are already about 85% full of blood, the atria contract and complete the filling of the ventricles. This final filling of the ventricles by atrial contraction is termed atrial kick. This effect is very important during exercise, when the volumes of blood returning to the heart are increased. Both atria contract essentially at the same time.
Ventricular function
Ventricles are pumping chambers which pump blood into the arteries. The left ventricle pumps blood into the main artery supplying blood to the body. This large vessel is referred to as the aorta. The right ventricle pumps blood into the main artery supplying blood to the lungs which is called the pulmonary artery (pulmonary always means to do with the lungs). Very shortly after the atria finish contracting, ventricular contraction begins. The ventricles start to contract from the cardiac apex, towards the base. This has the effect of directing blood towards the atrioventricular valves. In addition to contracting inwards the left ventricle shortens, pulling the cardiac apex towards the valves. As the ventricles start to contract, the pressure of the blood they contain increases. This increase in intraventricular pressure has the effect of closing the atrioventricular valves preventing blood from being pumped from the ventricles back into the atria. Both ventricles contract essentially at the same time.
It is interesting to note that ventricular contraction does not completely empty the ventricles. At the start of ventricular contraction (in a resting adult) a ventricle will contain 120mls of blood. During ventricular contraction 70mls of this will be ejected. This leaves 50mls of blood in the ventricle at the end of a contraction.
The cardiac cycle
A cardiac cycle is one complete contraction and relaxation of the heart. It describes the events which take place during one heart beat. The heart contracts at a regular rate from about eight weeks after conception until the death of the individual. Resting heart rate varies with the age of the person from about 140 at birth to around 110 at age two, 80 at age ten to around 70 in adults.
Systole and diastole
Systole refers to contraction of the myocardium. Atrial systole describes contraction of the atrial myocardium and ventricular systole is contraction of the ventricles. Diastole refers to the rest of the time when the myocardium is not contracting and therefore describes the resting phase of each cardiac cycle. In a cardiac cycle ventricular systole immediately follows atrial systole.
During ventricular diastole the ventricles fill with blood prior to the next contraction. There is then a period of systole when the ventricles are actively contracting. During a cardiac cycle ventricular systole takes 0.3 seconds and ventricular diastole about 0.5 seconds. As heart rate increases, for example during exercise, the length of diastole decreases.
Systolic blood pressure is generated as a result of ventricular contraction during ventricular systole. As the left ventricle pumps blood around the whole body, relatively high pressures must be generated. However, as the right ventricle only has to pump blood to the lungs only relatively low pulmonary arterial blood pressures are required. This explains why a typical blood pressure in the systemic circulation is 120/80 mmHg whereas in the pulmonary circulation it is 25/8 mmHg. The first figure represents the blood pressure in the arteries during ventricular systole and is referred to as the systolic pressure. The second figure is the pressure in the arteries when there is no active ventricular contraction during diastole. This second pressure reflects the elasticity of the arterial system and is termed the diastolic pressure. These principles explain why the wall of the left ventricle contains a much greater muscle mass than the right ventricle. The atrial walls are also relatively thin, as they only have to pump blood from an atrium into a ventricle.
Heart sounds
Both atrioventricular valves close at the same time, making a sound referred to as a ‘lub’. The closure of the two arterial semilunar valves makes a ‘dub’. These are termed the first and second heart sounds, so the normal heart should make a lub dub, lub dub, lub dub. Heart sounds can easily be heard with a stethoscope. Additional sounds may be abnormal and are often caused by disturbances in the smooth flow of blood. An abnormal heart sound, referred to as a ‘whoosh’, is often heard in septal defects where there is a communication between the right and left sides of the heart (a hole in the heart). The resultant mixing of oxygenated and deoxygenated blood reduces the efficiency of the circulatory system. In this case some oxygenated blood is returned to the lungs and some deoxygenated blood is pumped into the systemic circulation. Such conditions are usually congenital and often require surgical correction.
Blood circulation through the lungs and around the body
The heart is actually two pumps in one; there is a body pump and a lung pump. The left side pumps blood to the body (the systemic circulation) and the right side to the lungs (the pulmonary circulation).
As the left ventricle contracts blood is ejected into the aorta. From the aorta blood passes, via the arterial system, to perfuse all the tissues of the body. As the blood circulates through the capillaries of the body it gives up oxygen to the tissues. Veins then collect the blood and return it towards the heart. The systemic veins drain blood into two large central veins called the superior and inferior vena cava. These two veins drain the top and bottom halves of the body respectively. The superior and inferior vena cava then drain directly into the right atrium.
From the right atrium the blood passes through the tricuspid valve into the right ventricle. When the right ventricle contracts this causes the closure of the tricuspid valve and the opening of the pulmonary valve. This means blood will be pumped into the pulmonary artery, and on to the lungs. Back flow from the pulmonary artery into the right ventricle is prevented by the pulmonary valve. Shortly after leaving the right ventricle, the pulmonary artery divides into two main branches, one to each lung.
Blood is pumped to the lungs to be oxygenated and to excrete (excrete just means to get rid of) carbon dioxide. Haemoglobin in red blood cells absorbs oxygen from the lungs. This oxygenated blood will then return to the left side of the heart via the pulmonary veins. The four pulmonary veins, two from each lung, drain blood into the left atrium. From the left atrium, blood passes through the bicuspid valve into the left ventricle.
The order of the circulation of the blood can therefore be summarised as follows; left ventricle - aortic valve - aorta - body - vena cava - right atrium - tricuspid valve - right ventricle - pulmonary valve - lungs - pulmonary vein - left atrium - bicuspid valve - left ventricle. Both sides of the heart contract together, simultaneously pumping blood to lungs and body.
Arterial blood in the systemic circulation is bright red because it is rich in oxyhaemoglobin which is a bright red pigment. This is because the blood has passed through the lungs and is fully oxygenated. An oxygen saturation probe indicates that arterial blood in a healthy person is usually 98-99% saturated with oxygen. However, in the pulmonary arteries, the blood is on the way to the lungs to be oxygenated, after giving up much of its oxygen to the tissues of the body. This is why blood in the pulmonary arteries is dark red and deoxygenated. Blood in the systemic veins is dark red, compared to blood in the pulmonary veins which is bright red and fully oxygenated.

Diagram 2.5 This simplified diagram shows the flow of the blood through the heart and around the body and the lungs. You may find it helpful to colour these diagrams in. The tradition is red for oxygenated blood and blue for deoxygenated.

Diagram 2.6 This diagram shows more detail of the flow of blood around the systemic circulation. Arrows indicate direction of blood flow.
Circulation of blood through the coronary arteries
The first two arteries to leave the aorta are the right and left coronary arteries. These subdivide and supply blood to all of the smaller coronary arteries which perfuse the myocardium with blood. As this blood perfuses the myocardium it supplies the nutrients and oxygen essential for energy production and contraction. Disease of these arteries is termed coronary artery disease and is the single most common cause of death in most developed countries. This disease occurs when the lumen of the arteries is clogged up with a fatty cholesterol based material called atheroma. Because the atheroma blocks off part of the lumen, less blood is able to get through to the myocardium. This reduction in blood supply is called ischaemia. In addition, the atheroma increases the probability that a blood clot may form in the lumen of the artery, a pathological condition referred to as thrombosis. Clinically these consequences of atheroma may cause angina and myocardial infarction.

Diagram 2.7 The main coronary arteries as seen from the front. Coronary arteries are relatively thin arteries, partly explaining why they are prone to blockage in coronary arterial disease. The circumflex branch of the left and the right coronary artery carry on around the back of the heart to perfuse the posterior wall with blood.
This is a great way to educate lay people about the heart and circulatory system!
Good show!😄
Have you seen this more modern understanding of the heart - the work on the "helical heart" https://www.youtube.com/watch?v=v75tpamodY4